This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In today’s digitalized healthcare environment, keeping the best outcomes for patients at the center of all activity increasingly depends on the smart use of medical data. Access to a consolidated overview of healthdata empowers patients to better manage their conditions and participate more in their healthcare.
At the University of California Irvine Sue & Bill Gross School of Nursing, faculty members are developing ways for artificial intelligence to help deliver better patient care and improved outcomes. But amidst this confusion lies a potential solution: personalized healthdata.
The pandemic accelerated the need for these solutions, driven by many older individuals’ preference to age gracefully at home rather than moving to assisted living facilities or nursing homes. As use of digital healthtechnologies grows, ensuring patient privacy and data security becomes crucial.
doctors and nurses alike, are considering leaving their current role in the next two to three years. That 1 in 2 clinicians is significantly greater than the global 37% of physicians and nurses thinking about leaving their roles in the next 3 years, according to the report Clinician of the Future 2023 from Elsevier.
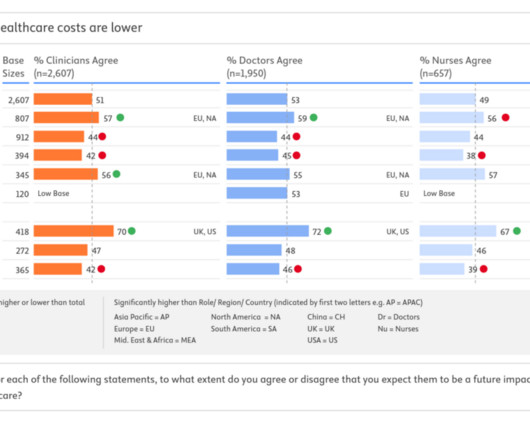
More younger doctors recognize the “immediate value” of telehealth, Philips found: 61% of younger doctors said telehealth was among the top digital healthtechnologies that would have most improved their experience during the pandemic. Philips presented more granular data for each of the five countries studied.
Being Philips, what underpins that quality and experience is technology; Philips explored telehealth, AI, digital health records (DHRs), and other digital health tools that can engage patients. 84% of consumers with access to personal electronic healthdata want their health care professionals to have access, as well.
Although HIPAA does not impose specific requirements regarding where healthdata must be stored, the amendments to the Act require qualifying health care providers in Florida to only store health records in the U.S., healthdata) to foreign jurisdictions. It also includes “ health care practitioners ” (e.g.,
Traditional risk scoring systems are also often cumbersome and impede clinical workflow by requiring patient data to be manually input by the examining physician. Predictions made by these tools use individual healthdata and are reflections of an individual’s dynamic health processes. risk score.
Stey’s Viewpoint recognizes that the drive real change in healthcare that impacts peoples’ health, it’s critically important to connect healthcare providers to the new-new innovations. Consumers-patients highly trust their doctors, their nurses, their pharmacists, above all professions in the U.S.
This article addresses key harms and biases associated with the SDOH technology movement, and provides suggestions to address these issues going forward. The Age of SDOH Technology. These needs are often documented within a screening tool developed by the health system or a technology vendor responsible for the SDOH referral platform.
Deloitte concludes that consumers still want the benefits of in-person health care services — personalized relationships with clinicians. For consumers to share the intimate asset of their personal healthdata, the situation requires trust.
"As we completed the evaluation process and selected the Enterprise Healthtechnology, the COVID pandemic struck and we had to immediately pivot our focus to COVID response – both for our own employees and in support of our employer clients." to a Northwell nurse," he said. " PROPOSAL.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content