This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
OSF HealthCare, a health system that serves Illinois and Michigan, had a big challenge: Managing the high rate of patient readmissions from hospitals to skilled nursing facilities and eventually to home care. THE PROBLEM This issue stemmed largely from gaps in continuous care during transitions between these settings.
This structured framework ensures that recommendations are practical, easily implementable, and aligned with the workflows of care teams. Applications in CareTransition The three principles of responsible AI use are particularly applicable in caretransitions, where managing patient handoffs between different care settings is critical.
For example, if your academic health sciences center has 40 clinical subspecialties across a dozen medical and surgical departments, and you populate your provider advisory council with only seven physicians, nurse practitioners and physician assistants to guide a massive clinical transformation – good luck to you!
“On hospital discharge and transition to the next level of care, older adults continue to face risks such as miscommunication, gaps in care and medication-related issues,” the researchers wrote. Transitionalcare models are designed to address these challenges with the primary aim of preventing readmissions.”
Analytic expertise is required to help prevent “information overload” and provide healthcare professionals with the tools for integrating and using the data for the betterment of that patient. From a patient´s perspective, digital health applications foster interaction between care teams and patients.
However, workers on both the providing and receiving ends of patient transfers are often overburdened with administrative processes and technological inefficiencies that bog them down and prevent them from doing higher-value clinical work. In the past, caretransitions have often come with concerns about risk and uncertainty.
Many, particularly those in skilled nursing facilities (SNFs), share this concern. With an estimated need for 191,000 additional nurses and a price tag of around $6.8 With an estimated need for 191,000 additional nurses and a price tag of around $6.8 While well-intentioned, the unfunded mandate presents a multifaceted problem.
However, workers on both the providing and receiving ends of patient transfers are often overburdened with administrative processes and technological inefficiencies that bog them down and prevent them from doing higher-value clinical work. Prior to that, he held nursing leadership and paramedic positions at West Tennessee Healthcare.
All of these capabilities support better caretransitions, which Fischer calls “one of the biggest gaps in health care.”. When a patient needs a walker, for instance, a nurse must order the walker, then get a physician to sign the order. Without that signature, the home health agency does not get reimbursed.
Effective communication during caretransitions, along with proper medication reconciliation, is vital for preventing readmissions and improving overall patient outcomes. Preventing Complications and Infections Preventing complications and infections is essential to reducing hospital readmissions.
ACO Accountable Care Organizations. CBCM Community Based Care Management Program. CDC Centers for Disease Control and Prevention. PH-MCO Physical Health Managed Care Organization. USPSTF United States Preventative Services Task Force. APM Alternative Payment Model. CBO Community Based Organization.
The aim of such an initiative is to smooth workflows, reduce unnecessary churn, and prevent data stagnation. One extremely forward-thinking provider organization designed an innovative program several years ago to transition reimbursement away from fee-for-service and towards value-based care.
. – The strategic deployment will provide Prisma Health and its Clinically Integrated Network, inVio Health Network , with real-time patient intelligence across the entire care continuum. By doing so, they can truly become an integrated extension of our care team, enabling us to deliver better outcomes and lower costs.”
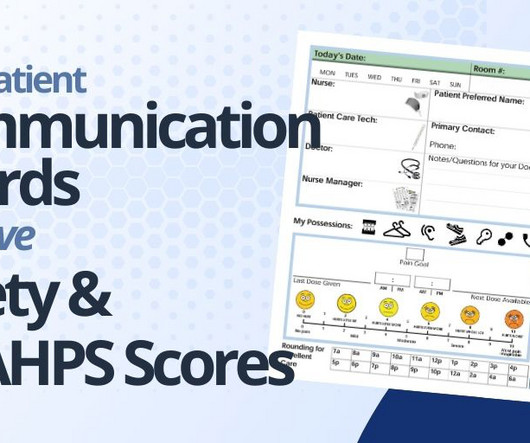
PATIENT SAFETY: Patient communication boards improve patient safety in hospitals in several ways: Enhance Communication Between Patient and Care Team: These boards enhance communication between patients, nurses, doctors and other hospital staff by providing a consistent visual and accessible means of conveying important information.
People with serious and life-threatening health conditions experience care needs that drive costs, including hospital admissions , emergency department utilization , and nursing home care. Kelley and Bollens-Lund, 2018. billion on chronic obstructive pulmonary disease (COPD) per year.
His school nurse can stay up-to-date regarding his medications. 2) Furthermore, Sara Heath writes about the importance of educating patients in an effort to cut down on hospital readmissions in her article, “Patient Engagement Strategies That Prevent Hospital Readmission.”
CHW services could be used for many health conditions as long as there is a care plan in place written by a physician, physician assistant, nurse practitioner, or a certified nurse midwife. Many provider types may supervise CHWs, including physicians, dentists, public health nurses and mental health professionals among others.
We at the Patient Safety Movement Foundation are known for our recognition of loved ones who have lost someone from preventable harm in healthcare. However, we also very strongly support the heroic efforts of our healthcare workers as we seek solutions to the system faults that lead to preventable errors occurring. For example, H.R.
MMRCs analyze these deaths that occur in their state each year and make recommendations to prevent them. [5] 5] These suggested changes often target individuals, hospitals, providers, and the broader health care system. Due to the pandemic, prenatal care visits decreased and maternal mental health conditions increased. [7]
To appropriately address SDoH, hospitals require care coordination technology to proactively consider these roadblocks to care and connect patients with local home- and community-based organizations to reduce patients’ reliance on hospitals and prevent avoidable visits and admissions.
Shared Plan of Care. Care Coordination Workforce. CareTransitions. health plans, providers, families of CYSHCN) in using, adapting, and implementing the National Care Coordination Standards for CYSHCN to develop or improve care coordination systems. Family understanding and access to care plan.
Paid Family Caregiving Colorado Colorado allows family members of Medicaid-enrolled CYSHCN to be paid for providing care to their children by becoming licensed as certified nursing aides. 25, 26 At the provider level, workforce shortages among professionals who deliver specialized pediatric care (e.g.,
The Master Plan also aligns with some of the governor’s key initiatives, such as the “California for ALL” vision and the Task Force on Alzheimer’s Prevention and Preparedness. Key findings of the Summary Assessment highlight inequities preventing Ohioans, especially older Ohioans, from living a long and full life.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content