This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
OSF HealthCare, a health system that serves Illinois and Michigan, had a big challenge: Managing the high rate of patient readmissions from hospitals to skilled nursing facilities and eventually to home care. THE PROBLEM This issue stemmed largely from gaps in continuous care during transitions between these settings.
This structured framework ensures that recommendations are practical, easily implementable, and aligned with the workflows of care teams. Applications in CareTransition The three principles of responsible AI use are particularly applicable in caretransitions, where managing patient handoffs between different care settings is critical.
The Research Institute for Home Care (RIHC) helped support the research. The goal of the SOAR program is to provide a high-quality, nurse-led replicable transition of care framework from hospital to home. It’s a really interesting model, and it’s really important to look at how to bridge those gaps in caretransitions.”
For example, if your academic health sciences center has 40 clinical subspecialties across a dozen medical and surgical departments, and you populate your provider advisory council with only seven physicians, nurse practitioners and physician assistants to guide a massive clinical transformation – good luck to you!
What You Should Know: – Radial Analytics , a Concord, MA-based company optimizing patient caretransitions with real-time decision-support solutions for payers and providers, today announced it has raised $3M in funding led by Initialized Capital. Such opportunities to intervene often occur at caretransitions.
And because of the pandemic, I think there was a rapid adoption to care in alternative sites. There were many seniors who would not want to go into a nursing home because nursing homes were hit so hard with COVID-19. We were able to say, “Okay, what is the next phase post-COVID around these trends with care in the home?”
Ashley Franks, Chief Nursing Informatics Officer at TigerConnect Nurses, the backbone of the medical field, have been facing a critical threat: burnout. A worrying 29% of nurses reported feeling like they’re at their wits’ end several times a week or even daily.
Facilitating close collaboration and communication across care teams as well as with patients helps achieve better and more timely outcomes. From a patient´s perspective, digital health applications foster interaction between care teams and patients.
Transitions of care involving seniors — especially those with multiple chronic conditions — can be risky. Despite this, there are a number of methods skilled nursing facilities (SNFs) and other health organizations can adopt to improve the transition from inpatient care to home for patients and their caregivers.
For home-based providers, maximizing the seamlessness of a post-hospital caretransition is paramount. RML Specialty Hospital — a long-term acute care hospital that offers critical care — has seen this firsthand through its utilization of the care coordination platform CarePort, which is a WellSky-owned company.
Patient transitions from the hospital to post-acute care providers, including home health agencies, continue to be plagued by incomplete medical records and missing information. Gaps in post-acute caretransitions are so common, in fact, that the U.S.
For example, a hospital case manager may have to send faxes and make phone calls to multiple skilled nursing facilities (SNFs) within the hospital’s network to identify which facility is most prepared to accept a given patient. In the past, caretransitions have often come with concerns about risk and uncertainty.
Many, particularly those in skilled nursing facilities (SNFs), share this concern. With an estimated need for 191,000 additional nurses and a price tag of around $6.8 With an estimated need for 191,000 additional nurses and a price tag of around $6.8 While well-intentioned, the unfunded mandate presents a multifaceted problem.
IQVIA is conducting a survey for the HHS Office of the National Coordinator for Health Information Technology to assess skilled nursing facility (SNF) capabilities related to interoperability, electronically exchanging information across organizations and systems. Why participate?
Experience Care has built a powerful financial and clinical software solution that is integrated to streamline data management, save time, and deliver high quality care for skilled nursing, assisted living, and other long-term care facility residents.
For example, a hospital case manager may have to send faxes and make phone calls to multiple skilled nursing facilities (SNFs) within the hospital’s network to identify which facility is most prepared to accept a given patient. Prior to that, he held nursing leadership and paramedic positions at West Tennessee Healthcare.
As states navigate current fiscal constraints, state policymakers are focusing on helping older adults remain in home-and community-based settings for as long as possible while also potentially reducing costly hospital and nursing home services. Reconceptualizing Nursing Home and Assisted Living Service Models. Food: With nearly 9.7
Addressing transitionalcare is important because it is a time when patients are vulnerable. TransitionalCare: Moving patients from one care setting to another”, American Journal of Nursing , September 2008, [link] , accessed 24 April 2023. Kansagara D, Chan B, Harmon D, Englander, H. Valverde, P.A.,
Equitable access to home-based care is hampered by disparities affecting certain racial, ethnic and socioeconomic groups, posing a challenge that extends to educating patients and families about home-based care services, and identifying those with advanced illnesses sooner to maximize the benefits.
PACE is a Medicare and Medicaid program that helps keep people in their communities instead of nursing homes. Oftentimes, programs are run out of community-based centers with the support of in-home care providers and their staff. Axxess adds three executives to its leadership team. “I
All of these capabilities support better caretransitions, which Fischer calls “one of the biggest gaps in health care.”. When a patient needs a walker, for instance, a nurse must order the walker, then get a physician to sign the order. Without that signature, the home health agency does not get reimbursed.
PointClickCare has a longstanding history of partnering with C3HIE, including a joint effort with the Texas Health Services Authority (THSA) in 2022, which expanded the Emergency Department Encounter Notification (EDEN) network.
References : Under CalAIM, Medi-Cal managed care plans (MCPs) became responsible for providing LTSS services that were traditionally provided under fee-for-service (FFS) in January 2023. pdf On October 1, 2023, Virginia Medicaid combined its two managed care programs of Medallion 4.0
One extremely forward-thinking provider organization designed an innovative program several years ago to transition reimbursement away from fee-for-service and towards value-based care. The program rewarded LTSS facilities and nursing facilities for high-quality and efficient treatment of enhanced respiratory medical conditions.
One other interesting fact is if you go back to 2019 and look at skilled nursing referrals and home health referrals, there has been a huge shift away from skilled nursing towards home health. Whereas skilled nursing has actually gotten close to returning to the 2019 levels, but still is not moving at the same rate that home health is.
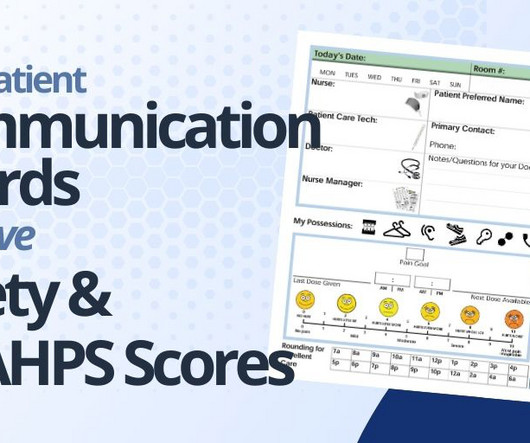
PATIENT SAFETY: Patient communication boards improve patient safety in hospitals in several ways: Enhance Communication Between Patient and Care Team: These boards enhance communication between patients, nurses, doctors and other hospital staff by providing a consistent visual and accessible means of conveying important information.
The Negatives Where there is much room for improvement is in the responsiveness of hospital staff (65% average HCAHPS score), communication about medications (61%), the quietness of the hospital environment (62%), and the patient’s caretransitions (51%).
. – The strategic deployment will provide Prisma Health and its Clinically Integrated Network, inVio Health Network , with real-time patient intelligence across the entire care continuum. By doing so, they can truly become an integrated extension of our care team, enabling us to deliver better outcomes and lower costs.”
Effective communication during caretransitions, along with proper medication reconciliation, is vital for preventing readmissions and improving overall patient outcomes. This program underscores the importance of improving caretransitions to minimize patient readmissions within a 30-day timeframe post-discharge.
Inside hospitals, for example, nurse case managers are the quarterbacks of care, wrangling insurance companies, providers, families, and physicians to find medical services for patients who need care following treatment for injury or illness. The SNF needs approved authorization before admitting a patient. About Russell Graney.
They are consequently significantly overrepresented in institutions, such as nursing facilities. They are also less likely to be employed or have a stable home , adequate medical care , and informal supports in the community. They live shorter lives and develop chronic health conditions earlier in life than other Americans.
Patient Perspectives on CareTransitions From Hospital to Home”, JAMA Network Open , 6 May 2022, [link] , accessed 19 March 2023 “Hospital discharge planning hinges on good communication”, Healthy Debate , 6 June 2017, [link] , accessed 19 March 2023 Minemyer, Paige. “The
His school nurse can stay up-to-date regarding his medications. He’s in developmental therapies at a private clinic several days a week and thanks to an effective EHR system, his physicians and therapists can be on the same page. We’re able to log his daily caloric intake through an EHR system.
In February 2022, for example, results from a nurse survey commissioned by a prominent staffing firm showed 56% of nurses reported that their mental health and well-being has suffered due to the pandemic, and 41% are considering leaving the profession for good. How Patient Flow Challenges Contribute to Burnout.
Shared Plan of Care. Care Coordination Workforce. CareTransitions. health plans, providers, families of CYSHCN) in using, adapting, and implementing the National Care Coordination Standards for CYSHCN to develop or improve care coordination systems. Family understanding and access to care plan.
By proactively addressing patients’ social-risk factors through technology, hospitals take a comprehensive and coordinated approach to whole-person care, resulting in better outcomes, lower costs, and sustainable care – all critical to success under value-based care models. Optimize skilled nursing facility length of stay.
In February 2022, for example, results from a nurse survey commissioned by a prominent staffing firm showed 56% of nurses reported that their mental health and well-being has suffered due to the pandemic, and 41% are considering leaving the profession for good. How Patient Flow Challenges Contribute to Burnout.
Enhance health team coordination and collaboration Care coordination is a complex process involving multiple stakeholders, including primary care physicians, specialists, nurses, and allied healthcare professionals. Modern care management platforms facilitate seamless collaboration and information sharing among care teams.
Paid Family Caregiving Colorado Colorado allows family members of Medicaid-enrolled CYSHCN to be paid for providing care to their children by becoming licensed as certified nursing aides. 25, 26 At the provider level, workforce shortages among professionals who deliver specialized pediatric care (e.g.,
People with serious and life-threatening health conditions experience care needs that drive costs, including hospital admissions , emergency department utilization , and nursing home care. Kelley and Bollens-Lund, 2018. billion on chronic obstructive pulmonary disease (COPD) per year.
CHW services could be used for many health conditions as long as there is a care plan in place written by a physician, physician assistant, nurse practitioner, or a certified nurse midwife. Many provider types may supervise CHWs, including physicians, dentists, public health nurses and mental health professionals among others.
CHW services could be used for many health conditions as long as there is a care plan in place written by a physician, physician assistant, nurse practitioner, or a certified nurse midwife. Many provider types may supervise CHWs, including physicians, dentists, public health nurses and mental health professionals among others.
Ensure access to referred services by coordinating behavioral health services with obstetric care, working with managed care organizations to guarantee members have access to specialists and treatment, addressing social determinants of health, and providing enabling services such as child care and transportation.
About the Lead Author Emerson Ea is clinical professor and associate dean for clinical and adjunct faculty affairs at New York University Rory Meyers College of Nursing. He is a 2022–2023 Health and Aging Policy Fellow working with the Administration for Community Living.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content