This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
OSF HealthCare, a health system that serves Illinois and Michigan, had a big challenge: Managing the high rate of patient readmissions from hospitals to skilled nursing facilities and eventually to home care. THE PROBLEM This issue stemmed largely from gaps in continuous care during transitions between these settings.
Applications in CareTransition The three principles of responsible AI use are particularly applicable in caretransitions, where managing patient handoffs between different care settings is critical. About Matt A. Murphy Matt A.
The new solution addresses the significant issue of hospital readmissions among Medicare beneficiaries. Coupled with the Centers for Medicare & Medicaid Services’ (CMS) increased focus on seamless caretransitions, Medicare Advantage plans are under pressure to intervene quickly and effectively to prevent avoidable readmissions.
The transition between hospital discharge and home health care is often fraught with issues. Unfortunately, it also happens to be one of the most crucial parts of a patient’s care journey. When I’m talking about acuity creep, I’m thinking about how much need do the patients in our care models require?”
Analytic expertise is required to help prevent “information overload” and provide healthcare professionals with the tools for integrating and using the data for the betterment of that patient. Failure to adhere to guidelines can increase the risk of complications, drive up costs, and lengthen hospital stays [5].
With over 50 locations in Canada, Right at Home will now leverage Sensis care copilot to augment their in-person care, detect early health risks and reduce hospitalizations and readmissions. Sensi.AI: Transforming Senior Care Through AI-Driven Insights Sensi.AI billion annually. Notably, 8.5%
Using the evidence-based UCSF Care Ecosystem model , trained CHWs reach out by phone and email to people with dementia and their caregivers one or more times per month over a six-month period. The CHWs provide support, education, and resources on coping with stress, preventing injuries, staying healthy, and connecting to community services.
Hospital readmissions can be costly and challenging for both healthcare providers and patients. By providing timely follow-ups, addressing patient concerns, and offering support post-discharge, medical call centers play a vital role in bridging the gap between hospitalcare and recovery.
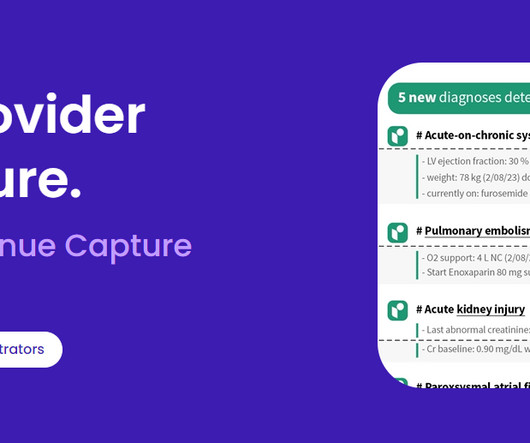
What You Should Know: – WakeMed Health & Hospitals and Regard today announced a 3-year enterprise agreement to deploy Regard’s AI clinical automation tool to the system’s 3 acute carehospitals by the end of 2024. ”
Lane Wise, Director of Customer Success, ABOUT Healthcare For patients, every transition of care to a different facility brings the risk of complications. Like many things in life, successful transitions of care often start with strong communication.
“We recognized that more quickly than a lot of providers, just because of the referrals we got from hospitals,” Myers said. “We We had a much higher percentage of managed care referrals coming our way, and we didn’t have the resources to care for those patients, and we wanted to care for them.
Lane Wise, Director of Customer Success at ABOUT Healthcare For patients, every transition of care to a different facility brings the risk of complications. Like many things in life, successful transitions of care often start with strong communication.
As the COVID-19 virus and its rapidly developing variants continue to disrupt the home health care industry , the need for home health providers continues to grow, with patients, payers and providers all seeing the benefits of moving care into the home. With that shift comes an increased need for better care collaboration.
The goal of the PHE was to help low-income people receive appropriate preventive and primary care during the pandemic without disruptions in coverage. However, the demand for healthcare is only going to rise, driven by the long-term impacts of Covid-19 and delaying care for other health conditions.
Birth of Telemedicine The genesis of telemedicine can be traced back to Boston during the late 1960’s with the birth of a fully functioning telemedicine system operating between Mass General Hospital (MGH) and the Logan Airport Medical Station. Benjamin Franklin said it best: an ounce of prevention is worth a pound of cure.
ACO Accountable Care Organizations. CBCM Community Based Care Management Program. CDC Centers for Disease Control and Prevention. PH-MCO Physical Health Managed Care Organization. USPSTF United States Preventative Services Task Force. APM Alternative Payment Model. CBO Community Based Organization.
. – The strategic deployment will provide Prisma Health and its Clinically Integrated Network, inVio Health Network , with real-time patient intelligence across the entire care continuum. Discharge Summaries : Improves communication by addressing challenges in sharing vital patient information across different healthcare settings.
People with serious and life-threatening health conditions experience care needs that drive costs, including hospital admissions , emergency department utilization , and nursing home care. Kelley and Bollens-Lund, 2018. billion on chronic obstructive pulmonary disease (COPD) per year.
The aim of such an initiative is to smooth workflows, reduce unnecessary churn, and prevent data stagnation. The acceleration of the value-based caretransition isn’t slowing; the good news is, it’s not too late to get started.
2) Furthermore, Sara Heath writes about the importance of educating patients in an effort to cut down on hospital readmissions in her article, “Patient Engagement Strategies That PreventHospital Readmission.”
A proliferation of point solutions add value in terms of data collection, but many are tacked onto IT architectures and siloed, resulting in data gaps or cumbersome manual data processing and integration, preventing timely and nuanced data analysis. Where does patient engagement fit?
And it’s becoming harder and harder for patients to get appointments with their PCP or the specialists they have been referred to for advanced care. When it is mismanaged, patients are delayed important care and providers are missing out on significant volume and revenue increases.
The state has used Medicaid waivers, and state plan amendments to pay for these services, as well as other mechanisms like hospital budgets and grants. Christiana Care’s Health Ambassador Program is funded through the federal Maternal, Infant and Early Childhood Home Visiting (MIECHV) program.
In addition, only four models met the requirements to be expanded in duration and scope: Home Health Value-Based Purchasing Model; Pioneer ACO Model; Repetitive, Prior Authorization of Repetitive, Schedule Non-Emergent Ambulance Transport Model; and Medicare Diabetes Prevention Program Expanded Model.
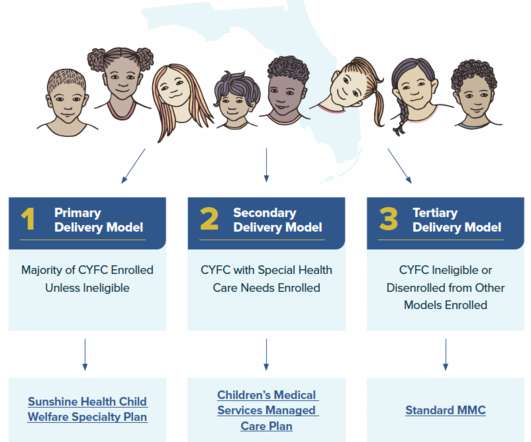
13] , [14] Moreover, few CYFC with behavioral health needs receive treatment in home or community-based settings, with many accessing care in more restrictive, residential settings (e.g., residential congregate settings or inpatient psychiatric hospitals). [15] personal care items or electronics). One-time financial stipends.
Hospitals are increasingly turning to value-based care initiatives to transform care delivery, lower the total cost of care, and improve patient outcomes. the number of patient visits), providers are reimbursed based on the quality of care delivered in value-based care. Reduce hospital admissions.
In the wake of the pandemic and growing consumer preferences, the hospital-to-home movement is gaining traction among health systems. Amidst bullish forecasts for the promise of hospital-to-home discharges, the ability for many patients to make this migration would be a difficult bridge to cross.
We at the Patient Safety Movement Foundation are known for our recognition of loved ones who have lost someone from preventable harm in healthcare. However, we also very strongly support the heroic efforts of our healthcare workers as we seek solutions to the system faults that lead to preventable errors occurring. For example, H.R.
MMRCs analyze these deaths that occur in their state each year and make recommendations to prevent them. [5] 5] These suggested changes often target individuals, hospitals, providers, and the broader health care system. Due to the pandemic, prenatal care visits decreased and maternal mental health conditions increased. [7]
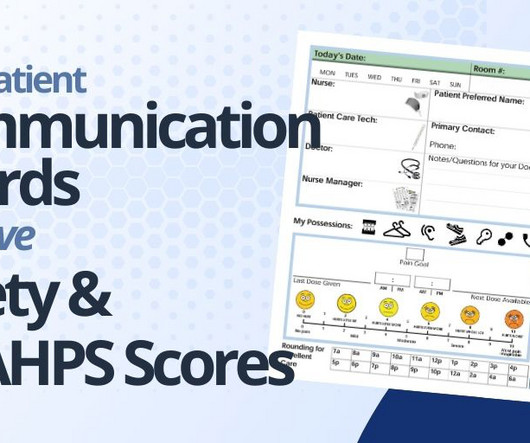
Patient communication boards play a pivotal role in enhancing both patient satisfaction and a hospital's HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score and star rating. Do you ever question the effectiveness of your hospital's communication boards?
Shared Plan of Care. Care Coordination Workforce. CareTransitions. health plans, providers, families of CYSHCN) in using, adapting, and implementing the National Care Coordination Standards for CYSHCN to develop or improve care coordination systems. Engagement in new services or caretransitions.
From streamlining documentation processes to facilitating care coordination between SNFs and hospitals, AI holds promise in alleviating the burdens faced by healthcare professionals. Moreover, it fosters connections and interoperability, paving the way for smoother caretransitions and reduced readmission rates.
The UVA health system also manages the Care Connection for Children center in SWVA, which is a statewide network funded through the Title V CYSHCN program, to provide care coordination services to CYSHCN and their families. 27] Children’s Hospital Association. Medicaid.gov. 26] State of Hawaii, Department of Health.
Acting on these insights could improve member experience, knowledge, and enable interventions that prevent future problems, improve outcomes, and drive down healthcare costs. This application of AI enables a scalable approach to proactive care at the population level, a cornerstone of VBC.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content