This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
First, consider the big health economics picture painted in the paper US Health Care Spending by Race and Ethnicity. The table arrays data the researchers analyzed from 2002 to 2016, identifying patterns of six types of medicalservices used by race and age group.
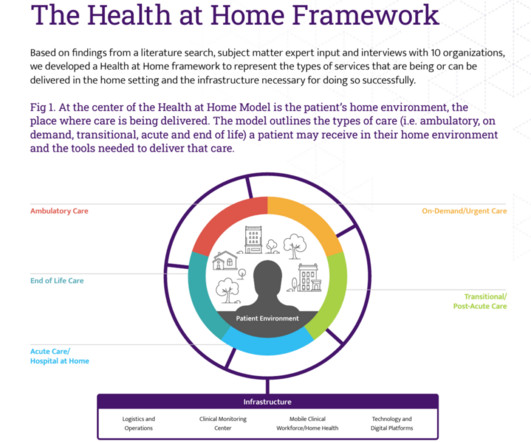
.” The H-a-H Framework is illustrated here, with the patient’s home environment is positioned at the center of the circle which identifies various careservices including: Ambulatorycare, covering primary care, chronic care, specialty care, mental and behavioral health, oncology-at-home, dialysis, infusion On-demand and urgent care, which (..)
This effect is an example of the “demand-induced supply” of medicalservices (Shih & Tai-Seale, 2011 ), which has been studied in the context of prescription drugs… … as patients…may choose which physicians to consult, they establish connections between physicians. An important finding.
In almost all of these 13 states a large portion of the population lives in rural areas, which are more likely than urban areas to have a shortage of primary care providers (PCPs). The Healthy Connections Value Care program went live July 1, 2021, and requires participation for PCCM providers. Health Aff (Millwood) 38 (12): 1993-2002.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content