This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The Transforming Episode Accountability Model (TEAM), which would eventually be mandatory if finalized, would have selected acute care hospitals put under full responsibility for the cost – and quality – of care from surgery up until the first 30 days after hospital discharge.
CMS’s strategic refresh initiative aims to meet five objectives: drive accountablecare, advance health equity, support care innovations, improve access and affordability, and establish partnerships to achieve these objectives. These models encourage providers to work together to coordinate care with a focus on quality.
“Primary care must be supported as the hub of integrated service delivery, with an emphasis on delivering preventive care and coordinating services through the various settings and specializations. Having person-centered metrics versus tracking activity-centered tasks will tell us that we are delivering true quality of care.
“Primary care must be supported as the hub of integrated service delivery, with an emphasis on delivering preventive care and coordinating services through the various settings and specializations. Having person-centered metrics versus tracking activity-centered tasks will tell us that we are delivering true quality of care.
The “National Forum on Advancing High-Quality, Equitable Care Coordination for Children and Youth with Special Health Care Needs” centered on two key topics for improving care coordination systems for CYSHCN: integratedcare coordination and the care coordination workforce.
The five strategic objectives for advancing this systemwide transformation include (1) Drive AccountableCare, (2) Advance Health Equity, (3) Support Innovation, (4) Address Affordability, and (5) Partner to Achieve System Transformation. Strategic Objective 1: Drive AccountableCare.
State health reform efforts increasingly focus on providing comprehensive and well-coordinated care to people with serious illness to improve quality of care and drive down costs. The state began implementation of palliative care legislation with an analysis of state Medicaid claims and encounter data.
In many states, SHIPs serve as the driving mechanism for engaging health care systems and communities in statewide planning, implementation, and evaluation efforts. Key examples include: Washington state established nine regional Accountable Communities for Health.
From 2015 to 2018, Colorado Medicaid operated the enhanced primary care medical provider (PCMP-E) program, which rewarded those PCCM providers (referred to in Colorado as PCMPs) that met at least five of nine enhanced factors with a $0.50 Value care organizations may participate under a risk or shared savings only option.
(NYSE: EHAB) has been active in the value-based care space. The company has a small – but growing – number of value-based contracts on the Medicare Advantage (MA) side, as well as AccountableCare Organization (ACO) partnerships. Integrated Home Care Services is a driver of value-based care in the home.
Urban residents generally have more choices regarding providers and facilities, while those in rural areas face challenges such as longer travel distances, limited provider availability and potential concerns about the quality of care.
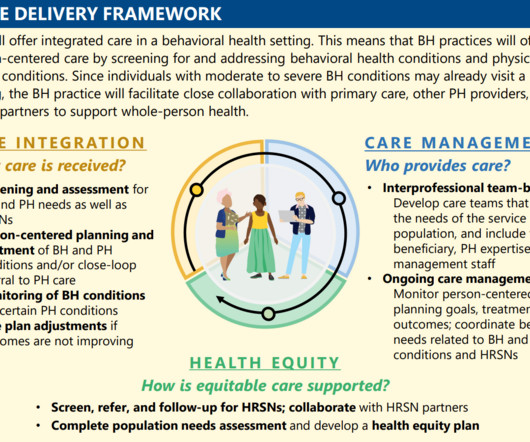
By focusing on integratedcare, addressing social determinants, and promoting health equity, the IBH Model has the potential to significantly improve the lives of millions of Americans. Performance-based incentives will further encourage quality improvement throughout the implementation period.
Worse, it would do so based on flawed economic theory, artificially narrow geographic markets, out-of-context quotations from a handful of documents, and with zero regard for the actual improvements to patient satisfaction and quality of care that would flow from the transaction.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content