This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Data is everywhere, but not always available or decipherable to help manage myriad challenges. Progress toward accountablecare is halting. Financial and revenue cycle disruptions are significant. Relentless cyberattacks are an ongoing threat. But still there are reasons to be cheerful.
The TNAP program is designed to accommodate stakeholders that will exchange data, including QHINs, other health information networks, health information exchanges, accountablecare organizations, data registries, labs, providers, payers, vendors, and suppliers.
Medicare Shared Savings Program: AccountableCare Organizations (ACOs) found to be blocking information may be excluded from the program for at least a year, forfeiting potential revenue. Those entities face potential civil monetary penalties of up to $1 million per violation.
Therefore, unlocking the correct data–at the individual patient and population levels–is critical to reversing this crisis. If providers could easily and securely access dynamic and actionable behavioral healthdata, they could develop more effective treatment plans based on a patient’s complete history.
One thing that has remained constant, though, is the organization’s push towards a value-based healthcare system. For Signify, the recent completion of its Caravan Health acquisition — an accountablecare organization (ACO) manager — is a major move toward driving more participation and success in value-based payment arrangements. “We’re
Kimura’s contributions as we chart a course toward care integration, new payment models, interoperability and transparent quality measures.”. Dr. Kimura is a practicing primary care internist with a specialization in clinical informatics.
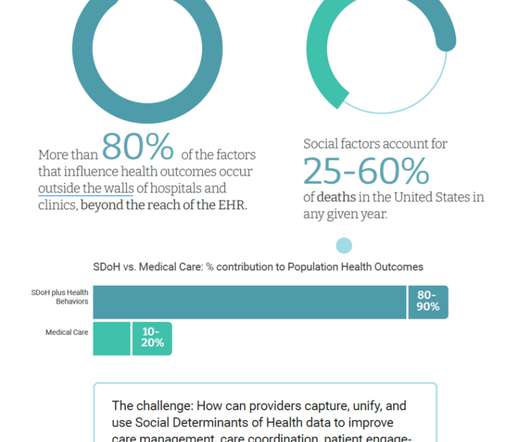
This is a transition phase wherein the vanguard systems are investing in digital transformation, but many not leveraging the SDoH data in population health programs yet by, say, integrating the determinants of healthdata in clinical workflows or using software to identify at-risk patients.
Collaboration aims to drive coordinated care and improve quality while reducing costs NS-EEH will strengthen its clinically integrated network (CIN) by incorporating Lumeris’ population healthdata platform into its value-based care strategy.
Behavioral health, said Cindy, doesn’t necessarily have to be integrated into the delivery system, but assessments should be integrated (e.g., PHQ-9’s may be administered by primary care providers), so that the behavioral healthdata may be integrated into the analytics framework used to manage population health.
A new Moms & Babies data mart is in development to allow Illinois Department of Public Health (IDPH) to access Medicaid enrollment and claims data. This will allow IDPH to link specified Medicaid data with other public healthdata systems and to independently analyze data related to maternal and infant health.
In the 1996 HIPAA statute (which covered a lot of other ground), Congress gave itself one year to legislate standards for healthdata privacy and security, and decreed that if it were to fail to meet that deadline, HHS would have to create regulations from whole cloth. Let’s start with the care coordination question.
In the 1996 HIPAA statute (which covered a lot of other ground), Congress gave itself one year to legislate standards for healthdata privacy and security, and decreed that if it were to fail to meet that deadline, HHS would have to create regulations from whole cloth. Let’s start with the care coordination question.
Behavioral health, said Cindy, doesn’t necessarily have to be integrated into the delivery system, but assessments should be integrated (e.g., PHQ-9’s may be administered by primary care providers), so that the behavioral healthdata may be integrated into the analytics framework used to manage population health.
Behavioral health, said Cindy, doesn’t necessarily have to be integrated into the delivery system, but assessments should be integrated (e.g., PHQ-9’s may be administered by primary care providers), so that the behavioral healthdata may be integrated into the analytics framework used to manage population health.
Behavioral health, said Cindy, doesn’t necessarily have to be integrated into the delivery system, but assessments should be integrated (e.g., PHQ-9’s may be administered by primary care providers), so that the behavioral healthdata may be integrated into the analytics framework used to manage population health.
Behavioral health, said Cindy, doesn’t necessarily have to be integrated into the delivery system, but assessments should be integrated (e.g., PHQ-9’s may be administered by primary care providers), so that the behavioral healthdata may be integrated into the analytics framework used to manage population health.
The partnership will be activated with an initial focus on migrating clinical workflows to NeuroFlow’s registry, or caseload management tool, providing care team members with the ability to track and measure patient progress in between appointments and improve resource allocation.
This feedback, along with state-collected healthdata, helped shape Oregon’s five priority areas : institutional bias; adversity, trauma, and toxic stress; behavioral health; access to equitable preventive services; and economic drivers of health.
In Rhode Island , the public health agency conducted a study to better understand the capacity of the CHW workforce, which includes parent consultants who provide care coordination for CYSHCN through the Rhode Island Parent Information Network.[18] Leveraging Data and Technology. 2] Abdi, Fadumo M., pdf ; Toomey, Sara L.,
Edifecs and Empowered-Home announced a partnership to provide automated prior authorizations to medical associations, AccountableCare Organizations (ACOs), Independent Physician Associations (IPAs), medical groups, and home healthcare agencies. Edifecs Partners with Empowered-Home to Deliver Automated Prior Authorizations.
1, 2023, the accountablecare organization (ACO) “REACH” Model – which stands for “Realizing Equity, Access and Community Health” – will take its place. The increased focus on data is a reason to be encouraged by the new model, according to insiders. I think there will have to be,” he said. How will that adjust things?”.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content