This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
OKane also reflected on 35 years of qualityimprovement at NCQA, and announced her new Quality Talks podcast before joining Dr. Meena Seshamani, incoming Secretary of the Department of Health for Maryland, for a Fireside Chat about the future of health carequality. Details coming soon!
Primarycare case management (PCCM) programs are one of the oldest types of Medicaid managed care, but over time most states have shifted to use managed care organizations (MCOs) to deliver services to Medicaid participants. ii] Rural areas are highly likely to suffer from shortages of primarycare and other providers.
NCQAs person-centered outcome (PCO) measures continue to attract the interest of the qualityimprovement community: The measures were recently recommended for inclusion in the Merit-Based Incentive Payment System (MIPS) for Medicare. MIPS Value Pathways: Primarycare and neurology. Why Are PCO Measures Important?
The Innovation Center also released the Making CarePrimary (MCP) model and the GUIDE model this year, innovative solutions to achieve multi-payer alignment and focus on populations that have historically been underfunded in health care.
You’ll learn how TennCare transformed its primarycare delivery model using HEDIS ® measures and total cost of care to gauge success. You’ll see how their activities played out in a real-life use case of addressing racial disparities in severe maternal morbidity.
State Medicaid programs, behavioral health authorities, public health, departments of insurance, human and social service agencies, departments of education, departments of corrections, housing, and employment can collaborate to align overlapping efforts, align policies, and braid funding and accountability mechanisms.
As part of our drive to improve health equity , most toolkit resources are available in Spanish. Have you used the toolkit? Let us know how it’s going! We welcome your feedback. The post Fifth Free Tool in Kidney Toolkit Helps Fight Kidney Disease appeared first on NCQA.
For instance, risk adjustment occurs based on patient characteristics and social determinants of health collected before the start of an episode; the authors argue that risk adjustment could take into account clinical or social needs changes during an episode. The authors also argue for more reimbursement for information sharing activities.
These discussion forums generated many promising and innovative solutions including improving healthcare by integrating behavioral health with primarycare, pursuing strategies for reducing low-value care and increasing high-value care, and developing better metrics for measuring performance in alternative payment models.
These discussion forums generated many promising and innovative solutions including improving healthcare by integrating behavioral health with primarycare, pursuing strategies for reducing low-value care and increasing high-value care, and developing better metrics for measuring performance in alternative payment models.
The five strategic objectives for advancing this systemwide transformation include (1) Drive AccountableCare, (2) Advance Health Equity, (3) Support Innovation, (4) Address Affordability, and (5) Partner to Achieve System Transformation. Strategic Objective 3: Support Care Innovations.
The COVID-19 pandemic has upended health care in America, and as of this writing, is still raging on. A quick snapshot reveals how decades-long investments by CAPP groups to better integrate their care delivery systems is paying off. The patient experience also significantly improves when care is coordinated versus delivered piecemeal.
Partnerships are strongest when they are based on a collective impact model, focusing on a common vision and developing shared accountability. As a result, services were better aligned and the MCOs referred CYSHCN to the Title V CYSHCN program for care coordination given the program staff’s expertise in serving this population.
Employers also collectively shoulder the biggest share of national health care costs, which regularly rise faster on an annual basis than overall inflation. demanding more transparency from insurers and other intermediaries.
As utilization, measured by visits to primarycare and specialist doctors, dipped during the pandemic, providers who had invested largely in value-based care were better able to weather the storm and the economic downturn by having a consistent source of revenue despite low utilization. Another benefit of RPM?
This includes alignment across the state Medicaid and behavioral health administrations, including shared systems and shared accountability, and a unified contracting approach across all relevant state agencies to create a unified network. Colorado Colorado is engaged in multi-pronged behavioral health reform.
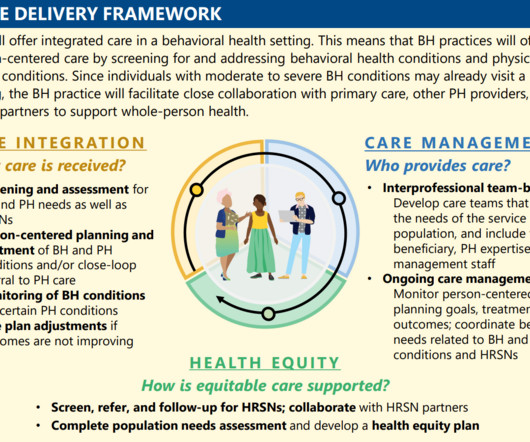
Integrated Primary and Behavioral Health Care A modern behavioral health system of care is fully integrated into the continuum of health care services, including primary and specialty care settings, and extends into homes and communities to ensure holistic and coordinated support.
of the Medicare fee-for-service population, homebound seniors aged 70 and older accounted for 11% of Medicare spending in 2015, according to the study. In light of these findings, the homebound represent a critically important population to target for qualityimprovement and reductions in Medicare spending.”.
On the other hand, a health plan may use the guide to implement a high-quality screening and assessment process through primarycare providers. Recruit providers to support system improvements. Conduct research on best practices for care coordination. Support qualityimprovement efforts. Social needs.
ACO AccountableCare Organizations. CBCM Community Based Care Management Program. NCQA National Committee for Quality Assurance. PCCM PrimaryCare Case Management. PH-MCO Physical Health Managed Care Organization. RAE Regional Accountable Entity. Acronym Guide. SPA State Plan Amendment.
Five conditions account for 39% of serious misdiagnosis-related harms: stroke, myocardial infarction, aortic aneurysm/dissection, spinal cord compression/injury, and venous thromboembolism. These figures are also consistent with diagnostic errors and harm rates in primarycare and inpatient settings.
The Department of Health Care Policy and Financing (the Medicaid program administrator) does not specifically require the Regional Accountable Entities (RAEs), care coordinating entities contracted with Colorado’s Medicaid program, or other managed care entities to cover CHW services, nor does the Department pay for CHW services under FFS.
Now, Oregon’s specialty court program and its staff will receive state-specific guidance, education, training, and peer review, among other qualityimprovement strategies. Connect individuals to health care access prior to release. Support drug court budgets with cross-systems resources. Leverage policy to support MOUD.
State leaders play a critical role in convening key internal and external partners, implementing engagement and input processes that foster shared ownership and accountability toward goals at the state and community levels.
The IBH Model aims to bridge the gap between behavioral and physical health by: Empowering community-based behavioral health practices: These practices, including mental health centers, opioid treatment programs, and safety net providers, will become the central point of care, offering integrated services for both mental and physical health needs.
First, issuers may only count provider incentive and bonus payments as claims expense if they are “tied to clearly defined, objectively measurable, and well-documented clinical or qualityimprovement standards.” Second, issuers only may count expenditures directly related to activities that improve healthcare quality.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content