This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Applications in CareTransition The three principles of responsible AI use are particularly applicable in caretransitions, where managing patient handoffs between different care settings is critical. Responsible, transparent and safe AI can be applied in real-world care management applications.
Home Care remains deeply fragmented, disconnected and too difficult to navigate,” Proffitt said Wednesday. “It It accounts for about $150 billion of the health sector today, and we expect this figure to climb substantially by the end of the decade. UnitedHealth Group’s (NYSE: UNH) Optum acquired LHC Group last year for $5.4
It’s a really interesting model, and it’s really important to look at how to bridge those gaps in caretransitions.” It also takes into account patient preferences and patient needs before care is transitioned. population begins to skew older, care coordination woes will exacerbate. As the U.S.
What You Should Know: – Bamboo Health , the leader in Real-Time Care Intelligence, is teaming up with Radial , a pioneer in decision support software for value-based care, to enhance care coordination and drive success in accountablecare.
He also noted that nearly all of the patients the organization will add in fully accountable value-based relationships this year will have access to support through its home-based care platform. “We Another way is through a focus on caretransitions. This year, we expect to make more than 2.5
While discharge communication directly with the patient drives most of these success metrics, the post-acute providers must also be well-informed so they can be accountable for the delivery of intended outcomes. In the past, caretransitions have often come with concerns about risk and uncertainty. vs. 49.5%).
Modern care management platforms facilitate seamless collaboration and information sharing among care teams. With care coordination, providers can more effectively orchestrate care, leading to improved caretransitions and reduced medical errors.
While discharge communication directly with the patient drives most of these success metrics, the post-acute providers must also be well informed so they can be accountable to the delivery of intended outcomes. vs. 13.5%), higher adherence to treatment regimen (86.1% vs. 79.0%), and higher patient satisfaction (60.9% vs. 49.5%).
The shift to value-based care. Connecting training with outcomes serves patients and staff, but the shift to value-based care means attention to outcomes is imperative as home-based caretransitions to rewarding providers for the quality of the care they deliver.
Measuring and Improving Performance: Organizations perform continuous quality improvement of their LTSS program and identify actionable steps to improve care for their members. CareTransitions: Individuals receiving LTSS experience smooth and safe transitions between care settings.
– Bamboo Health’s ACO partners succeed under value-based care programs like the MSSP by utilizing their Pings solution, which provides real-time visibility into patient admission, discharge, and transfer (ADT) care events. .
“I look forward to collaborating with our team and our colleagues at Optum as we enter a new phase of care delivery, explore new growth opportunities and seek new ways to achieve our mission of helping seniors live more fulfilling lives.”. Paul, Minnesota-based health care spending account (HSA) administrator.
rebalancing spending to improve access to home and community-based services, improving caretransitions, or encouraging greater care coordination) Innovative oversight approaches for Medicare/Medicaid integrated models What’s In It for States?
Message statuses such as “sent,” “delivered,” and “read” ensure accountability and clarity. Enhanced teamwork: Tailor real-time notifications to different roles, prioritizing information to facilitate rapid response and efficient collaboration, particularly during critical scenarios.
CMS’s strategic refresh initiative aims to meet five objectives: drive accountablecare, advance health equity, support care innovations, improve access and affordability, and establish partnerships to achieve these objectives. Why align specialty care with value-based models?
Streamlining Care and Empowering Providers WellSky envisions integrating AI tools into their solutions to automate repetitive tasks, freeing up valuable time for human interaction and personalized care.
Effective communication during caretransitions, along with proper medication reconciliation, is vital for preventing readmissions and improving overall patient outcomes. Recognizing these characteristics allows caregivers to craft individualized plans accounting for each patients particular risks and requirements.
The private health plans, which are an alternative to traditional Medicare, account for 42% of the total Medicare population. A study by the Kaiser Family Foundation found that four in five Medicare Advantage enrollees are in plans that require them to obtain authorization from insurers prior to receiving care. About Russell Graney.
No matter the practice’s type or patient volume, there are so many ways things can go wrong with a fax-dependent process that is nearly impossible to standardize, has no real built-in accountability and is dependent on significant levels of coordinated communication. Increase visibility into the patient’s care coordination.
States are hoping to achieve a number of goals with their MLTSS programs, including increasing access to home and community-based services, promoting care coordination, enhancing quality and beneficiary satisfaction, and mitigating cost growth.
There is a greater emphasis on care coordination and diminished focus on siloed, add-on remote monitoring solutions that simply mirror the fragmentation and unreliable caretransitions of our existing system.
Shared Plan of Care. Care Coordination Workforce. CareTransitions. health plans, providers, families of CYSHCN) in using, adapting, and implementing the National Care Coordination Standards for CYSHCN to develop or improve care coordination systems. Accountable Person. Domain 2: Shared Plan of Care.
The Negatives Where there is much room for improvement is in the responsiveness of hospital staff (65% average HCAHPS score), communication about medications (61%), the quietness of the hospital environment (62%), and the patient’s caretransitions (51%). Plus many more strategies.
The five strategic objectives for advancing this systemwide transformation include (1) Drive AccountableCare, (2) Advance Health Equity, (3) Support Innovation, (4) Address Affordability, and (5) Partner to Achieve System Transformation. Strategic Objective 1: Drive AccountableCare.
CAQH CORE (Committee on Operating Rules for Information Exchange) conducted years of research and identified key opportunity areas in the industry that could smooth the implementation of value-based care payments, making communication between payers and providers more effective and sustainable.
In addition to a range of metrics related to promoting prevention and reducing utilization related to ambulatory care-sensitive conditions, ICSP measures have included advanced care planning, evidence of physician order for life-sustaining treatment (POLST), effective caretransitions, and assessment and management of chronic pain.
ACO AccountableCare Organizations. CBCM Community Based Care Management Program. PCCM Primary Care Case Management. PH-MCO Physical Health Managed Care Organization. RAE Regional Accountable Entity. In addition, CHWs are often included in Accountable Communities for Health (ACH). Acronym Guide.
In July 2022, Maine launched the first phase of its new PCPlus initiative, which is an APM through MaineCare, Maine’s Medicaid program, that provides a higher per member per month (PMPM) rate for a whole-person care approach that includes services such as care coordination, health and oral screenings, and caretransition.
The receptionist who answered the phone informed me I could set up an account through their online patient portal and retrieve all of the notes taken during his appointment, as well as contact his doctor, and review his medical records.
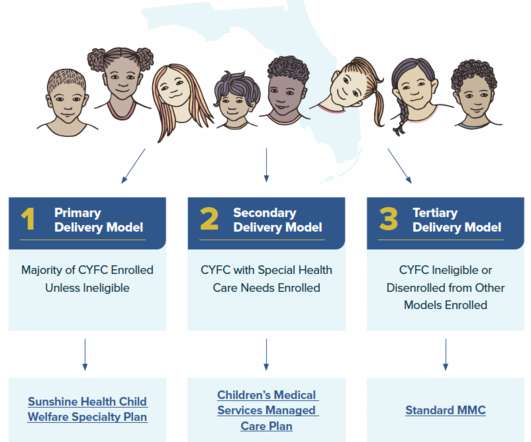
Additionally, many specialized MMC programs require the contracted MMC entity to meet certain reporting and quality benchmarks, which may include documentation of services provided and timeliness of those services, health outcomes, or foster care-specific performance improvements. personal care items or electronics). 17] Ibid. [18]
Outside of the SPA context, Massachusetts met with CHW interested parties to better understand how to support CHWs (which could be supported with Delivery System Reform Incentive Payment Program funding paid to accountablecare organizations authorized through the state’s previous 1115 Demonstration Waiver, rather than a SPA).
The Department of Health Care Policy and Financing (the Medicaid program administrator) does not specifically require the Regional Accountable Entities (RAEs), care coordinating entities contracted with Colorado’s Medicaid program, or other managed care entities to cover CHW services, nor does the Department pay for CHW services under FFS.
The result is setting up in advance very predictable role accountabilities, clear technology-enabled processes, and best practices to optimize the transfer operations while reducing workforce stress. There are patient flow barriers that come up frequently in the acute care management of patients.
Equipped with the right tools, providers can make the appropriate post-acute care decision for their patients to mitigate readmission risk and reduce potential post-acute care spending. As touched on above, post-acute care delivered in the SNF setting accounts for a significant portion of Medicare fee-for-service costs.
These barriers are revealed in research conducted by a team from the University of Michigan (my alma mater) published in JAMA (May 6, 2022), Patient Perspectives on CareTransitions From Hospital to Home. “We need to start respecting and accounting for unpaid caregivers.
The result is setting up in advance very predictable role accountabilities, clear technology-enabled processes, and best practices to optimize the transfer operations while reducing workforce stress. There are patient flow barriers that come up frequently in the acute care management of patients.
We organize all of the trending information in your field so you don't have to. Join 19,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content